

How Is Maniscus Tear Repaired
Original Editor - Rachael Lowe, Melissa Decoen, Céline Vankeerberghen
Top Contributors - Nikkie Dassen, Melissa Decoen, Rachael Lowe, Admin, Marlies Schils, Oyemi Sillo, Kim Jackson, Vidya Acharya, Mathieu Vanderroost, WikiSysop, Hans Vanhaelen, George Prudden, Simisola Ajeyalemi and Adam Vallely Farrell
Definition/Clarification [edit | edit source]
A meniscal repair is a surgical process to repair a torn meniscus via keyhole surgery. It is a minimally invasive process often undergone as an outpatient. Factors affecting success include tear age, location and design, age of the patient, as well equally any associated injuries.
Clinically Relevant Anatomy [edit | edit source]
Medial meniscus
Lateral meniscus
The major meniscal functions are to distribute stress beyond the knee during weight bearing, provide shock absorption, serve as secondary joint stabilizers (in an anterior cruciate ligament scarce knee, menisci will serve as articulation stabilizers [1] , provide articular cartilage nutrition and lubrication, facilitate joint gliding, forestall hyperextension, and protect the joint margins. 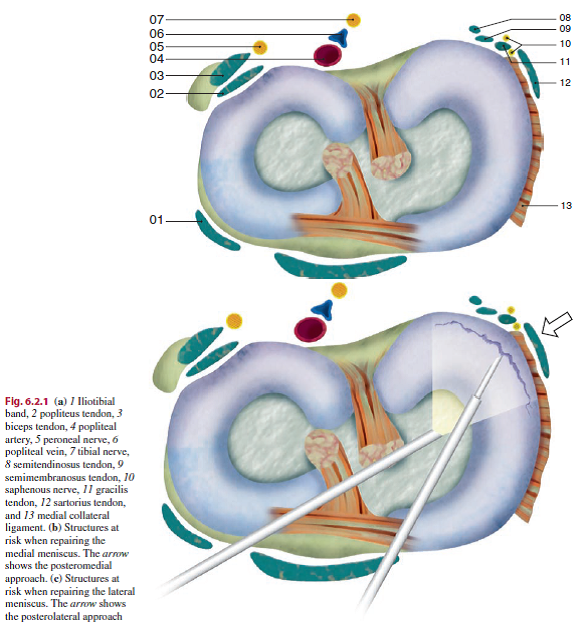
During knee flexion, the femoral condyles glide posteriorly on the tibial plateau in conjunction with tibial internal rotation. The lateral meniscus undergoes twice the anteroposterior translation of the medial meniscus during human knee flexion. This translation prevents the femur from contacting the posterior margin of the tibial plateau.[2]
The meniscus is divided into three zones: the red-red, the red-white and the white-white. The zones are divided by vascularization and thus healing potential.The red-red zone is the peripheral zone of the meniscus. It is very proficient vascularized and has a expert healing rate. Patients differ in vascularization of the medial and lateral meniscus, varying between xx-30 and 10-25 % width. The red-white zone is the heart third with less vascularization but can though heel sometimes. The white-white zone has no blood capillaries at all and therefore cannot heal. 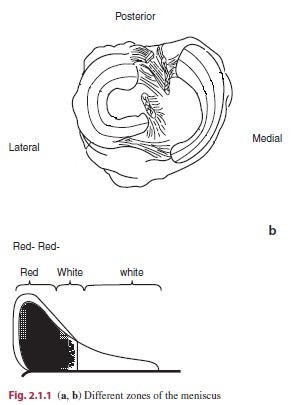
Epidemiology [edit | edit source]
Meniscal lesions are the most common intra-articular knee injury in the United States and are the most frequent cause of surgical procedures performed by orthopaedic surgeons. The mean almanac incidence of meniscal lesions is 0.066 %. [24] There are more male patients (59,5%) undergoing an isolated meniscal repair compared with female patients (40,5%). This is the same compared with male patients (60%) undergoing a concomitant meniscal repair and inductive cruciate ligament. And so most of the patients undergoing meniscal repair are males. [3]
In general, meniscal tears frequently occur in middle-anile and elderly patients and are caused past long term degeneration.
One third of the lesions by young patients are caused by sports-related injuries, because of the cutting or twisting movements, hyperextension or actions with great forcefulness. In more than 80%, meniscus tears are accompanied past anterior cruciate ligament (ACL) injury.
Meniscal lesions in children are dissimilar than those in adult patients. In children, more 70 pct are isolated meniscal lesions caused more of the time past sport-related twisting of the knee joint. [4]
Indication for Procedure [edit | edit source]
Indication for procedure
Nonoperative treatment is rarely successful for treating meniscal tears in young athletes and repair of the torn menisci is often required[five]
Repair of a meniscal lesion should exist strongly considered if the tear is peripheral and longitudinal, with concurrent Anterior Cruciate Ligament (ACL) reconstruction, and in younger patients. The probability of healing is decreased in complex or degenerative tears, central tears, and tears in unstable knees. Numerous repair techniques are available.[6]
Preservation of meniscal tissue is recommended, regardless of age - in agile patients- whenever possible.[7]
Meniscal tears amenable to repair include unstable tears > ane cm in length and occurring in the outer 20% to thirty% toward the periphery, or in the so-called red-red zone. Those tears occurring more toward the junction of the red-white zone may also heal, and the conclusion to repair should be made based on the clinician's judgment. Platonic candidates for repair are vertical, longitudinal tears occurring within three mm of the peripheral rim.
Indication for surgery
The decision whether a lesion is treated surgically or non-surgically is the beginning decision made after definitively diagnosing a meniscal tear. This decision is based on patients factors (east.thousand. age, co-morbidities and compliance), tear characteristics (e.g. location of the tear, historic period of the tear and blueprint of the tear) and the fact whether the tear is stable or unstable. When the tear is unstable surgery is necessary.[vi]>
[7]>
A degenerative tear or a not-degenerative tear which is asymptomatic or stable is treated not-surgically. In the other cases, such as non-degenerative tears or tears which are symptomatic the tears are treated surgically. [7]
The second decision concerns whether meniscal repair or meniscectomy is appropriate. If none of the normal surgical treatments seems appropriate full meniscectomy is the terminal option. The factors that should have been taken in consideration while making decisions should be: 1) the clinical evaluation, 2) related lesions and 3) the exact type, location, and extent of the meniscal tear. [8]
If meniscal repair is performed combined with an ACL reconstruction the success charge per unit is influenced. Whether the influence is positive or negative is studied in several studies with dissimilar conclusions. [ii][five][6][7]
Tenuta JJ et al. also found that width of the lesion is an of import factor no lesion with a width of more than 4 mm healed.[5]
Differential Diagnosis [edit | edit source]
• Joint line tenderness and effusion. Withal the joint line tenderness test may be simulated positive with osteoarthritis, osteochondral defects, collateral ligament injury or fractures. [five]
Effusion may also occur when there are issues with the cruciate ligaments, basic or the articular cartilage.
• Symptoms are frequently worsened by flexing and loading the knee, activities such as squatting and kneeling are poorly tolerated. But it's the same with patients suffering from other pathologies like chondromalacia patellae, fractures and Sinding Larsen Johansson Syndrome.
• Complaints of 'clicking', 'locking' and 'giving way' are common. Patients as well complain about 'giving' fashion when at that place are suffering from inductive cruciate ligament injury. The feeling of instability and locking is too common with osteochondritis dessecans. 
Clinical Presentation [edit | edit source]
- Joint line tenderness and effusion.
- Symptoms are oftentimes worsened by flexing and loading the knee, activities such as squatting and kneeling are poorly tolerated.
- Complaints of 'clicking', 'locking' and 'giving way' are common
Diagnostic Tests [edit | edit source]
When making a diagnosis, relevant patient history, physical examination, and appropriate imaging studies are required.[5]
- Joint line tenderness has been reported to be the best common exam for meniscal injury.
- McMurray'due south test positive if a pop or a snap at the joint line occurs while flexing and rotating the patient's knee joint.
- Apley'southward examination performed with the patient decumbent, and with the examiner hyperflexing the knee joint and rotating the tibial plateau on the condyles.
- Steinman's test performed on a supine patient by bringing the human knee into flexion and rotating.
- Ege'southward Test is performed with the patient squatting, an aural and palpable click is heard/felt over the area of the meniscus tear. The patient'southward feet are turned outwards to notice a medial meniscus tear, and turned in to detect a lateral meniscus tear.
- Meniscal Imaging is an essential tool in decision making for surgical management of meniscus tears. Accurate imaging of the meniscus is essential to evaluate the damaged expanse and to select the most advisable handling. Imaging is too an important tool for postoperative management and treatment, follow up and identification of any farther injury. Currently, magnetic resonance imaging (MRI Scans) is the preferred imaging technique. Other techniques are Radiography, Computed Tomography (CT Scans) scan, Computed Tomography (CT) arthrography and Magnetic Resonance Arthrography. [1]
The advantages of MRI in the diagnosis of a meniscus lesion are: grade-I and grade-II tears are detected earlier, actress-articular structures are likewise visible, no radiation and MRI is a non-invasive imaging technique. [9]
Outcome Measures [edit | edit source]
An overall meniscal repair success rate of 85-90% has been found by R.P.Walter et al. [7]
Patients undergoing con concomitant anterior cruciate ligament reconstruction enjoyed significantly improved outcomes of meniscal repair. (91%), while those with a past history of anterior cruciate ligament reconstruction had significantly worse meniscal repair success rate (63%). Bohnsack establish a healing rate of 86-95%. The overall success rate for healing menisci with meniscal repair is high.[10]
In most of the studies they took a 2nd MRI to confirm whether the lesion is healed. A patient is considered as existence healed when at that place is no lesion on the second MRI and the patient is able to resume his normal life/activities.
Locked bucket-handle, meniscal tears heal at a high rate when repaired as an isolated surgery; even when total weight bearing and activeness before reconstruction is allowed and when the tear is in the white-on-white zone.[iii]
Age or fourth dimension between injury and surgery don't touch the amount of people that were healed by meniscal repair.[iv]
Medical Management [edit | edit source]
Indications [edit | edit source]
Indication for surgery are complete or large incomplete longitudinal tear of the media and lateral meniscus close to the base, large flap tear, so-called bucked-handle tear. [eleven]
Contra-indications [edit | edit source]
Degenerative meniscal tissue. Unstable genu joint without concomitant surgical stabilization. Complex meniscal tears or radial tears, tear in the central avascular region, gonoarthrosis, joint infection and local peel disorders. [11]
Surgical Techniques [edit | edit source]
Meniscal repairs tin can be performed past open, inside-out, outside-in and all-inside techniques. But not all meniscus tears have the ability to heal, the meniscal tear design and the presence of acceptable vascularity are both central. [12]
When meniscus repair is carried out nether arthroscopic visualization, in the same manner equally the inside-out, the outside-in and the all-inside technique, some common steps, which are independent of the technique, accept to be followed. In that location have to be arthroscopic ready-upwardly, tear debridement and fixation. [13]
Open up technique [edit | edit source]
This technique offers the advantage of better preparation of the tear side. However, only the most peripheral of tears in the red-scarlet zone are amenable to this technique and the main disadvantage of this technique is the take a chance of neural damage. Nowadays this technique isn't frequently used anymore.
The capsule is incised posterior to the collateral ligament and the synovium is opened to give direct access to the posterior segment of the meniscus and the tear, provided that it is a vertical peripheral longitudinal tear. In case of a horizontal tear, the meniscosynovial rim needs to be dissected in gild to expose the peripheral meniscal rim and the horizontal cleavage. [xiii][14]
Inside-out technique [edit | edit source]
This technique has been used commonly for tears in the posterior horn or the torso of the meniscus and the tears take to be in the red-red zone or in the red-white zone. [13][15][16]
Absorbable or nonabsorbable 2-0 or 0 sutures are passed from inside the genu to a protected area on the outside of the joint capsule, using long flexible needles. The sutures are retrieved through an extra-articular posteromedial or posterolateral incision. The posterior neurovascular structures are protected with a big retractor. The knots are tied outside the joint over the capsule. [13][14]
This technique has been considered the aureate standard in meniscus repair because of the proven long term results, but there is yet a gamble of neurovascular complications. [13][16][17]
Outside-in technique [edit | edit source]
This technique is used in the anterior horn of the meniscus and was initially designed to subtract the run a risk of neurovascular complications. [13][eighteen]
A cannulated 18-estimate spinal needle is passed across the tear from the exterior-in. Once the abrupt tip of the needle is in view, the suture is passed through the arthroscopic ipsilateral portal. An interference knot is tied in the cease of the suture and the suture is pulled back. The process is repeated and the free ends are tied 2 by two over the capsule through an accessory peel incision until the tear is stabilised. Sutures may be placed alternately on the femoral and tibial surface of the meniscus in order to residuum the repair. [13]
All-inside technique [edit | edit source]
This technique can exist used for repairing extreme posterior horn tears. All-within repairs have been traditionally carried out using several devices, such every bit staples, tacks and screws. Nearly of these devices are bioabsorbable and composed of rigid poly-50-lactic acid (PLLA). [thirteen]
[12][17][19]
The newest devices are the cocky-adjusting suture devices. They are based on the same principle every bit the other devices. An anchor is positioned behind the sheathing and a suture compresses and holds the axial meniscal office by using a sliding knot. These implants share the potential ability to deform and move with the meniscus during weight bearing and behave a lower risk of chondral abrasion. The devices are RapidLoc, FasT-Fix and the Meniscal Sure-fire. [13]
The advantages of all-within repair include ease of utilize, avoidance of an accompaniment incision, shorter operation time, less risk to neurovascular structures and especially for the suture devices better forcefulness. [13]
[12][19]
Complications [edit | edit source]
Minor [twenty] et al. studied the complications of x,262 patients undergoing meniscal repair. Of the 10,262 patients 1,68% had complications. These complications were: Hemarthrosis, infection, thromboembolic disease, coldhearted complications, musical instrument failure, reflex sympathetic dystrophy, ligament injury, fracture and neurologic injuries. With hemarthrosis being the most common complexity and neurologic injuries beingness to the lowest degree common. No vascular injuries were reported. And in that location was emphasized 7% incidence of saphenous neuropathy by Austin et al.[21]
Physical Therapy Management [edit | edit source]
Pre-Operative [edit | edit source]
During the pre-operative phase of total knee joint replacement and anterior cruciate ligament reconstruction, information technology is proven that quadriceps forcefulness preparation leads to improved knee function and a better quality of life after the performance. (LoE:1B)[4] (LoE:1)[8] (LoE:4)[ii]
It is as well proven that neuromuscular electrical stimulation improves quadriceps musculus strength in subjects with Human knee Osteoarthritis Most patients who choose for meniscal repair are operated within a brusk menstruum of time, because of that there is seldom pre-operative concrete therapy. But if a quick operative intervention is not possible for any reason, we presume that quadriceps grooming is also beneficial for patients undergoing meniscal repair.
Post-Operative [edit | edit source]
The employ of electromyographic biofeedback in the early stages of rehabilitation, after meniscal repair, helps patients to command their muscles. Information technology tin aid attain physical activities that crave better neuromuscular coordination and control. For these reasons one may consider electromyographic biofeedback as an important component of rehabilitation after meniscal repair. Electromyographic Biofeedback is not responsible for the degrees in hurting, swelling, or other post-operative symptoms. This technique is a painless, non-invasive method that tin exist used in muscle recovery. This technique tin can exist used in all phases of rehabilitation. [one]
The blazon of surgery employed is largely dependent on the type of tear and its location. The most common surgical lesion in the human knee is a torn meniscus[9] [22] The goal of the surgery is to save equally much as possible healthy tissue.[vii]
In, long term, the surgical repair of the meniscus gives a better result than a partial meniscectomy. But the revalidation is longer.[10] This is something that the athlete must choose whether he wants to resume the sport quickly or not.
Types of Surgical Repair [edit | edit source]
In that location are 4 types of surgical repair: open, inside-out, outside-in, and all-inside.
For each operation they have to remove the loose parts, both surfaces of the tear should be sanded and the vascularity should be encouraged.[10]
The all-within techniques are attractive because of the decrease in operative time and ease of the technique. Short-term results are positive for the all-inside technique; notwithstanding, good long-term data on these techniques are lacking.[1]
Patients who take repairs of peripheral meniscus tears are generally progressed more quickly than those who take repairs of tears extending in the central i-3rd region or those who undergo meniscal transplantation. [half-dozen]
The advantage of meniscectomy is that only the damaged tissue is removed. Important is that the circular collagen fibers may non be cut. [10] [3] When that happens, the meniscus will lose his function as distributor of weight and so there is an increased risk of Osteoarthritis.
A disadvantage of meniscectomy is that there is a prolonged conservative aftercare. There needs to be a period of maximum prognosis to obtain the all-time possible healing.
Patients who have had an arthroscopic partial meniscectomy often initially feel knee swelling, pain, and loss of range of motion (ROM), and they may have increased joint laxity and osteoarthritis in the long term.[4]
Meniscal injuries are often accompanied by injuries to the anterior cruciate ligament, the collateral ligaments or the joint cartilage. [8] [two] Such associated injuries as well influence functional recovery later an arthroscopic meniscectomy.(Level of Evidence: 3A) [five] [6] [7] [1]
Supervised rehabilitation afterwards surgery has been advocated and studied as part of short- and long-term follow-up afterwards arthroscopic partial meniscectomy. [4]
The goal of rehabilitation is to restore patient's office based on individual needs. Information technology is important to consider the blazon of surgical process, which meniscus was repaired, the presence of coexisting genu pathology (particularly ligamentous laxity or articular cartilage degeneration), the blazon of Meniscus rupture, the patient'southward age, preoperative human knee status (including time between injury and surgery), decreased range of motion or forcefulness, and the patient's able-bodied expectations and motivations. [nine] [x] [3]
Exercise has been suggested to be an efficient treatment for patients with human knee degeneration in social club to improve knee part and limit joint pain. At that place is strong prove that physical training plays an of import part in order to reduce symptoms, improve muscle forcefulness and physical ability.[four]
Important points in the therapy:
• command the pain and inflammation - Cryotherapy, analgaesics, NSAIDs,
• To regain good knee command [4]
• Restore ROM (Range of motion) [4]- ROM exercises within any limits in range that the consultant has requested [9]
• Restore the flexibility [iv]
• Restore musculus office [iv]- specific strengthening exercises including quadriceps (A medial meniscus lesion influences the force of the M. Vastus medialis.[8]), hamstrings, calf, hip
The practise program should consist of both concentric and eccentric exercises to receive muscular hypertrophy equally well equally neuromuscular function. [4]
• Optimize neuromuscular coordination - proprioceptive re-teaching
• Progress weight bearing - weight bearing and joint stress are necessary to enhance the functionality of the meniscal repair so should exist progressed as indicated by the consultant. Excessive shear forces may be disruptive and should be avoided initially.
Concrete practise 3 times weekly during 4 months could lead to more than 35% comeback of knee function.[4] Any rehabilitation program should be written on the patient's body, every patient is different and will react differently to the rehabilitation.
The results are for a large part depended on the speed and exactness of how the diagnosis is confirmed.
Unresisted open chain exercises should be given to patients who underwent meniscal repair. Because the study of David L. et al. supports that it does not place undue stress on meniscal repairs. (LoE:4)[10]
The findings of many studies support weight-bearing limitations during the initial four to eight weeks after meniscal repair.In theory, weight begetting alone should not disrupt healing meniscal tissue, because the hoop stresses are primarily absorbed at the periphery of the meniscus. However, weight bearing in conjunction with tibiofemoral rotation during human knee flexion, could produce shear forces capable of disrupting healing meniscal tissue.[two]
Standard 'cookbook' protocols should be avoided and individualized programs - based on the type of surgical procedure, which meniscus was repaired, the presence of coexisting articulatio genus pathology (ligamentous laxity or OA), meniscal tear type, the patient's historic period, preoperative kneestatus (including the fourth dimension between injury and surgery), loss of ROM and strength, and the patient'south athletic expectations and motivations – should be encouraged.
Accelerated meniscal repair rehabilitation programs that permit total human knee ROM and full weight bearing are becoming more than mutual, with return to full activity as early as 10 weeks later surgery.[two]
Key Research [edit | edit source]
add links and reviews of high quality evidence here (case studies should be added on new pages using the example study template)
Resources [edit | edit source]
| Arthroscopic meniscal repair from the Os and Articulation Dispensary of Houston[two] |
Timothy Brindle,John Nyland and Darren L. Johnson (2001) The Meniscus: Review of Bones Principles With Application to Surgery and Rehabilitation. Journal of Athletic Training, 36(2), 160–169.
References [edit | edit source]
- ↑ one.0 1.1 1.two one.3 i.iv Andrews S. et al., The shocking truth about meniscus, Journal of Biomechanics, 44(16): 2737-40, Nov 2022. Level of testify: 3A
- ↑ 2.0 2.ane ii.2 2.iii 2.4 ii.five 2.half-dozen Timothy Brindle,John Nyland and Darren L. Johnson (2001) The Meniscus: Review of Basic Principles With Application to Surgery and Rehabilitation. Journal of Athletic Preparation, 36(2), 160–169.
- ↑ 3.0 3.1 3.two three.3 de Loës One thousand., A 7-year report on risks and costs of knee injuries in male person and female youth participants in 12 sports, Scandinavian Journal of Medicine & Scientific discipline in Sports 2000: 10: 90-97. Level of show: 2A.
- ↑ 4.00 four.01 four.02 four.03 iv.04 4.05 4.06 4.07 iv.08 4.09 iv.10 4.11 Eleftherios A.M., The knee meniscus: Construction, function, pathophysiology, electric current repair techniques and prospects for regeneration, Elsevier, 2022. Level of evidence: 1A
- ↑ v.0 5.1 5.2 5.3 5.4 5.5 Poulsen MR, Johnson DL. Meniscal injuries in the young, athletically active patient. fckLRDepartment of Orthopaedic Sugery, Academy of Kentucky, Lexington, KY. Abstract.
- ↑ 6.0 six.1 half dozen.2 6.3 half dozen.4 Stärke C, Kopf S, Petersen West, Becker R. Meniscal repair. Arthroscopy. 2009 Sep;25(9):1033-44. Epub 2009 Feb 26. Abstract.
- ↑ 7.0 seven.ane vii.two seven.3 7.4 vii.5 seven.6 Heckmann TP, Hairdresser-Westin SD, Noyes FR. Meniscal repair and transplantation: indications, techniques, rehabilitation, and clinical outcome. J Orthop Sports Phys Ther. 2006 Oct;36(x):795-814. Abstruse.
- ↑ 8.0 eight.1 8.ii eight.three DeHaven Ke. Decision-making factors in the treatment of meniscus lesions. Clinical Orthopedics & Related Research 1990; (252) 49-54. Level of show: 5 (abstract)
- ↑ 9.0 9.1 9.2 9.3 Biedert RM., Intrasubstance Meniscal Tears: Clinical aspects and the office of MRI, Archives of Orthopaedic & Trauma Surgery 1993; 112 (3). Level of prove: 3B
- ↑ 10.0 x.one 10.2 10.3 10.4 10.5 Bohnsack M, Ruhmann O. Arthroscopic meniscal repair with bioresorbable implants. Operative orthopadie und Traumatologie. 2006; xviii (5-6). Level of evidence: ii
- ↑ 11.0 11.1 Bohnsack K, Ruhmann O. Arthroscopic meniscal repair with bioresorbable implants. Operative orthopadie und Traumatologie. 2006; xviii (5-half-dozen). Level of prove: two
- ↑ 12.0 12.1 12.2 F. Alan Barber et al., Meniscal repair techniques, Sports medicine and arthroscopy Review, Volume fifteen (4), Pages 199-207, december 2007
- ↑ 13.0 13.1 13.2 13.three 13.4 13.5 13.6 thirteen.seven thirteen.8 13.ix BEAUFILS, P. The Meniscus, Springer-Verslag, Berlin Heidelberg,2010,397
- ↑ 14.0 14.1 Due north. Maffulli et al., Meniscal tears, Open Admission Periodical of Sports Medicine, Volume 1, Pages 45-54, 2022
- ↑ Nam-Hong Choi et al., Comparison of Arthroscopic Medial Meniscal Suture Repair Techniques: Inside-Out Versus All-Within Repair, The American Periodical of Sports Medicine, 2009 Level of evidence: 2
- ↑ 16.0 xvi.ane C. G. Nelson et al., Within-Out Meniscus Repair, Arthroscopy Techniques, Volume 2, Issue 4, Pages e453–e460, november 2022
- ↑ 17.0 17.one K. A. Turman et al., All-Inside Meniscal Repair, Sports Wellness, Volume i (5), Pages 438–444, september 2009
- ↑ Trommel, M.F. Meniscal Repair, Thela-Thesis, Amsterdam,1999.
- ↑ 19.0 19.ane G. H. Yoon et al., Meniscal repair, Knee joint Surgery & Related Enquiry, Volume 26 (2), Pages 68-76, Juni 2022
- ↑ Pocket-size NC., Complications in arthroscopic surgery performed by experienced arthroscopists. Arthroscopy 1988; iv (3); 215-221.fifty. Level of evidence: 2
- ↑ Austin KS, Sherman OH. Complications of arthroscopic meniscal repair. Am J Sports Med 1993; 864-8; discussion 868-9. Level of evidence: 2
- ↑ Brent M,C.D, et: Event of early on active range of move rehabilitation on outcome measures afterward fractional meniscectomy; knee surg sports traumatol arthrosc (2009) 17: 607-616

Source: https://www.physio-pedia.com/Meniscal_Repair
Posted by: coulterunise1990.blogspot.com
0 Response to "How Is Maniscus Tear Repaired"
Post a Comment